
Rethinking Disability: From Medical Charity to Social Justice By Ashmita Singh
Student submission from the Introducing Critical Disability Studies: Indian Contexts, Global Perspectives online course.
I will be honest with you: I started this course thinking I already understood disability. I had good intentions, a rough idea of accessibility ramps and screen readers, and the vague sense that “inclusion” meant making room for people who were somehow different. The course dismantled all of that, gently but firmly.
What followed was one of the most genuinely unsettling and exciting intellectual experiences I have had in a while. This blog is my attempt to think through what I learned, what changed in me, and why it matters far beyond any assignment submission.
“Disability is not the problem. The problem is a world built for a narrow idea of what a human body and mind should be.”
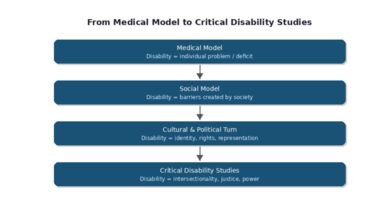
Before the course, I mostly understood disability through what scholars call the medical model. Disability, in this framework, is a deficit, a deviation from the normal body that needs to be fixed, managed, or accommodated. It is a problem located within the individual. What this course did, across every lecture and reading, was to shift that lens entirely.
Ableism Is Everywhere, and It Was Already in My Head
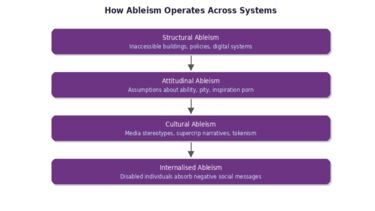
The lecture on Anti-Ableism in Teaching and Research was where things got uncomfortable in a productive way. The presenter made a point that I keep coming back to: universities are designed around an idealised notion of the “normal” body and mind. Speed, standardised testing, lecture-hall formats, timed exams, all of it assumes a particular kind of person.
The concept of access intimacy genuinely surprised me. It describes the quiet ease that disabled people feel when someone truly gets their access needs, not as a checklist item, but as a relational and emotional reality. It shifted my thinking away from the language of accommodation (which can sound like burden management) toward something much warmer and more human.
📌 Real-World Example: The Inaccessible Seminar Room A wheelchair user at a university is told their seminar has been moved to an “accessible” room. When they arrive, the room is accessible in name only: the projector cannot be lowered, the seating is fixed, and the acoustics make it impossible to follow conversation. Structural ableism and attitudinal ableism operate together, making the student feel like an afterthought rather than a full participant. |
I also began noticing how my own assumptions about productivity were shaped by ableist values. Society prizes efficiency and speed, and when those are your default standards, anyone who moves, thinks, or communicates differently is already at a disadvantage. Not because they lack ability, but because the system was never designed with them in mind.
Bollywood and the Politics of Feeling Seen
I did not expect a section on Bollywood to be one of the most critically sharp parts of the course. But the materials on disability representation in Indian cinema genuinely reframed how I watch films.
Michele Friedner's work on disability in urban India describes how disabled bodies are used to create what she calls “feel-good diversity”: emotional unity and national pride without any of the structural accountability that would make life actually better for disabled people. The image looks inclusive. The politics beneath it does not change.
🎬 Case Study: The Silent National Anthem Deaf children performing the Indian national anthem in sign language was widely celebrated as moving and patriotic. But the course asked a harder question: were these children being honoured as individuals with full rights, or were they being used as symbols of a feel-good narrative? Representation without structural change can actually entrench exclusion by making society feel it has already done the work. |
Priyam Sinha's research on “New Bollywood” added another layer. Screenwriters are increasingly using disability narratives because they are emotionally rich and relatively unexplored. Films like Taare Zameen Par genuinely raised public awareness about learning disabilities. But the course also helped me see the limits: supercrip stories (where disabled characters overcome their disability through sheer will), tokenism, and the persistent framing of disability as tragedy or triumph rather than as ordinary life.
Growing up, I consumed these narratives without question. I now understand that representation is not neutral. What we see on screen shapes what we think is possible, acceptable, and normal in real life.
“Representation matters not just because it makes disabled people feel seen, but because it teaches everyone else how to see them.”
Workplaces: Where ‘Reasonable’ Is Doing a Lot of Heavy Lifting
The WAARC project materials on inclusive work culture were sobering. Despite decades of disability rights legislation, disabled employees continue to face barriers in recruitment, promotion, and day-to-day workplace participation. The barriers are often not dramatic or obvious. They are the inaccessible intranet, the meeting that was not captioned, the culture where asking for adjustments feels like an admission of weakness.
💼 Case Study: Reasonable Adjustments in Practice A Deaf employee at a law firm requests live captioning for weekly all-staff meetings. The firm agrees but uses auto-generated captions with 60% accuracy. The employee misses critical information consistently but does not escalate because they fear being seen as difficult. The adjustment was technically provided; inclusion was not. This illustrates how ableist attitudes and inadequate implementation can undermine even well-intentioned policy. |
The concept of “reasonable adjustments” is interesting because of the word “reasonable.” Who decides what counts? The course made clear that accessibility is not charity or special treatment. It is about creating the conditions for equal participation. Flexible work, accessible digital systems, and supportive cultures benefit far more than just disabled employees.
What stayed with me most was the emphasis on co-production with Disabled People’s Organisations (DPOs). The principle is simple but radical: do not make decisions about disabled people without disabled people. This is not just good ethics; it produces better outcomes.
Research With, Not On: Rethinking Who Gets to Know
Before this course, I thought of research as something that happens to communities. Researchers arrive, observe, collect, interpret, and publish. The community gets a PDF they will probably never read. The course offered a very different vision.
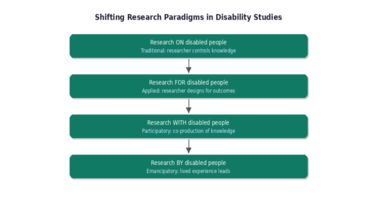
The shift from research ‘on’ disabled people to research ‘with’ and eventually ‘by’ disabled people is not just a methodological preference. It is a political commitment. It says that lived experience is a form of expertise, that disabled people are not passive subjects but active producers of knowledge.
🔬 Case Study: Participatory Action Research in Practice A research team studying employment barriers for autistic graduates invites autistic participants to co-design the interview questions, interpret findings, and present at the final conference. The resulting recommendations are grounded in lived experience and are far more actionable than what a traditional top-down study would have produced. The process itself becomes an act of inclusion. |
The discussion on vulnerability was something I needed to hear. Disabled people are routinely categorised as ‘vulnerable’ in research ethics frameworks. The course pushed back on this: vulnerability is not inherent to disability. It is produced by unequal social structures, power imbalances, and institutional failures. Framing disabled people as automatically vulnerable can reinforce the very paternalism that excludes them.
Arts-based and creative research methods were a genuine revelation. The idea that knowledge does not have to come packaged in academic prose, that stories, images, and emotions are legitimate ways of knowing, felt like it opened a door I had not known was closed.
Healthcare: When Care Itself Needs Care
The lectures on medical humanities and disability in healthcare were perhaps the most personally affecting part of the course for me. Medicine has historically positioned itself as the solution to disability. But the course traced how medical frameworks have also pathologised, institutionalised, and erased disabled lives.
🏥 Case Study: Disabled Medical Students and Classroom Ableism Disabled medical students have reported hearing their professors make casual comments suggesting that certain diagnoses automatically mean a poor quality of life. These comments are not just hurtful; they shape clinical practice. A doctor who believes that disability equals suffering will make different decisions than one who understands disability as a dimension of human diversity. What is taught in medical schools matters beyond the classroom. |
Narrative medicine stood out as a framework I want to carry forward. The idea that a doctor’s ability to listen to a patient’s story, to understand their context, their values, their fears, is as clinically important as knowing their test results felt obvious once I heard it. And yet, it is so rarely how medicine is actually practised.
“What would healthcare look like if it started from the assumption that every patient is the expert on their own life?”
I also found myself thinking about the disabled medical professionals who contributed to these sessions. They were not just sharing data; they were modelling something. A doctor who has navigated the healthcare system as a disabled person brings knowledge that no textbook can provide. Their presence in the profession is not a concession; it is an asset.
What I Am Taking Forward
If I had to name the single biggest shift this course produced in me, it would be this: I used to think of inclusion as something we do for disabled people. I now understand it as something we build together, or not at all.
Critical Disability Studies is not a niche subfield. It is a framework for understanding how power, culture, bodies, and institutions interact. Every system we design, every research question we ask, every story we tell, encodes assumptions about who counts as normal, who gets to participate, and who is left to adapt.
I am not claiming I have shed all my ableist assumptions. I am certain I have not. What I have, though, is a vocabulary and a habit of questioning that I did not have before. I notice things I used to walk past. I ask questions I used to think were unnecessary. That feels like the beginning of something.
Disability is not the problem. Our collective failure to imagine and build a world for all of us is.
References
Friedner, M. (2017). How the disabled body unites the national body: Disability as ‘feel good’ diversity in urban India. Contemporary South Asia, 25(4), 347–363. https://doi.org/10.1080/09584935.2017.1369516
Goodley, D., & Singh, S. Introduction to Critical Disability Studies [Lecture slides]. University of Sheffield.
Ktenidis, A. Anti-Ableism in Teaching and Research [Lecture slides]. University of Sheffield.
Lee, C. How medical humanities can help challenge ableism and expand inclusion in healthcare [Lecture slides]. University of Sheffield.
Mishra, A., & Hayden, N. Inclusive Research Methods [Lecture slides]. University of Sheffield.
Palaniappan, D. Setting the Context: Emergence of DPOs in Indian Disability Movement [Lecture slides]. University of Sheffield.
Sinha, P. (2023). Scripting disability as the ‘new’ Bollywood: Pitching, reflecting, researching and negotiating. Media, Culture & Society. https://doi.org/10.1177/01634437231177080
Soorenian, A. Co-Producing an Inclusive Work Culture: Challenges and Opportunities [Lecture slides]. University of Sheffield.

iHuman
How we understand being ‘human’ differs between disciplines and has changed radically over time. We are living in an age marked by rapid growth in knowledge about the human body and brain, and new technologies with the potential to change them.